Practice
Core exercises
A VRT programme is built from four modules. Each engages a different recovery mechanism; a real plan blends them by deficit and progresses each as the patient tolerates more demand.
- X1 viewing
- X2 viewing
- progress sitting → standing → walking
- repeat provocative positions
- busy-environment exposure
- VR / simulator
- Romberg / tandem on firm vs foam
- head-turn walking
- dual-task gait
- sit-to-stand
- stairs & reaching
- aerobic walking / cycling
A · Gaze stabilisation
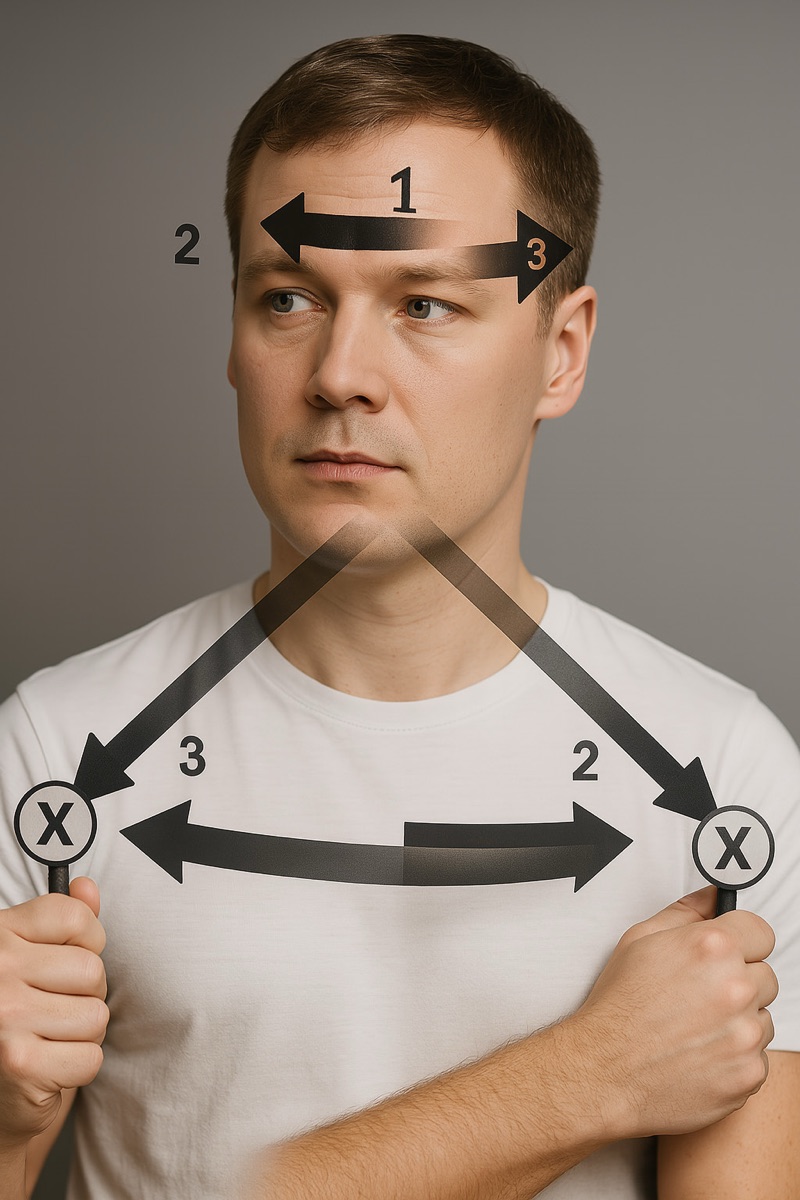
These exercises steady the vision. The patient keeps their eyes on a target — a letter on the wall — while moving the head. Doing this a little every day teaches the eyes to stay locked on, so the world stops bouncing.
Gaze stabilisation recalibrates the VOR using two exercises. In X1 viewing, the patient fixates a stationary target while moving the head side-to-side or up-and-down, generating retinal slip. X2 viewing moves target and head in opposite directions for a greater demand, introduced once X1 is mastered. Progress from sitting to standing to walking, and add background complexity and head speed.1
The dose-limiting variable is symptom tolerance, not repetitions: brief, frequent bouts (e.g. 1–2 minutes, several times daily) sustain the retinal-slip stimulus without over-provoking. Gains in dynamic visual acuity track functional recovery, so re-test DVA to titrate difficulty.1
B · Habituation
For dizziness provoked by specific movements or visual scenes, habituation desensitises through controlled exposure. Identify the provocative motions — lying down, rolling over, rapid head turns — and practise them deliberately, typically 3–5 repetitions, two to three times daily, with brief rests, over 7–10 days until the response wanes. Warn patients that mild, temporary worsening is expected and is the point.2

C · Balance & gait training
Balance work engages the vestibulo-spinal pathways and sensory reweighting. Begin with static stances — Romberg, single-leg, tandem — on firm then foam surfaces, eyes open then closed. Progress to dynamic tasks: walking with head turns, over obstacles, and at varied speed and direction. Dual-task training (walking while counting backwards) restores the automaticity that daily life demands and reduces falls.3


D · Functional & endurance training
Functional tasks rebuild independence: sit-to-stand drills, stair negotiation, reaching, and turning. Endurance work — treadmill or outdoor walking, stationary cycling — reverses deconditioning, supports neural recovery and builds tolerance for the more demanding modules. Integrated with the other three, this delivers a holistic, multi-domain programme.


Key points
- Four modules: gaze stabilisation, habituation, balance & gait, functional & endurance.
- X1 fixates a stationary target; X2 moves target and head oppositely — progress X1 → X2.
- Habituation provokes mildly and deliberately; a transient flare is expected.
- Balance training scales by surface, stance, visual input and dual-tasking.