Practice
Assessment & outcomes
Accurate assessment is the foundation of VRT — it classifies the deficit into gaze instability, motion sensitivity or postural imbalance, each of which points to a different exercise module. The same tools, repeated, track progress.
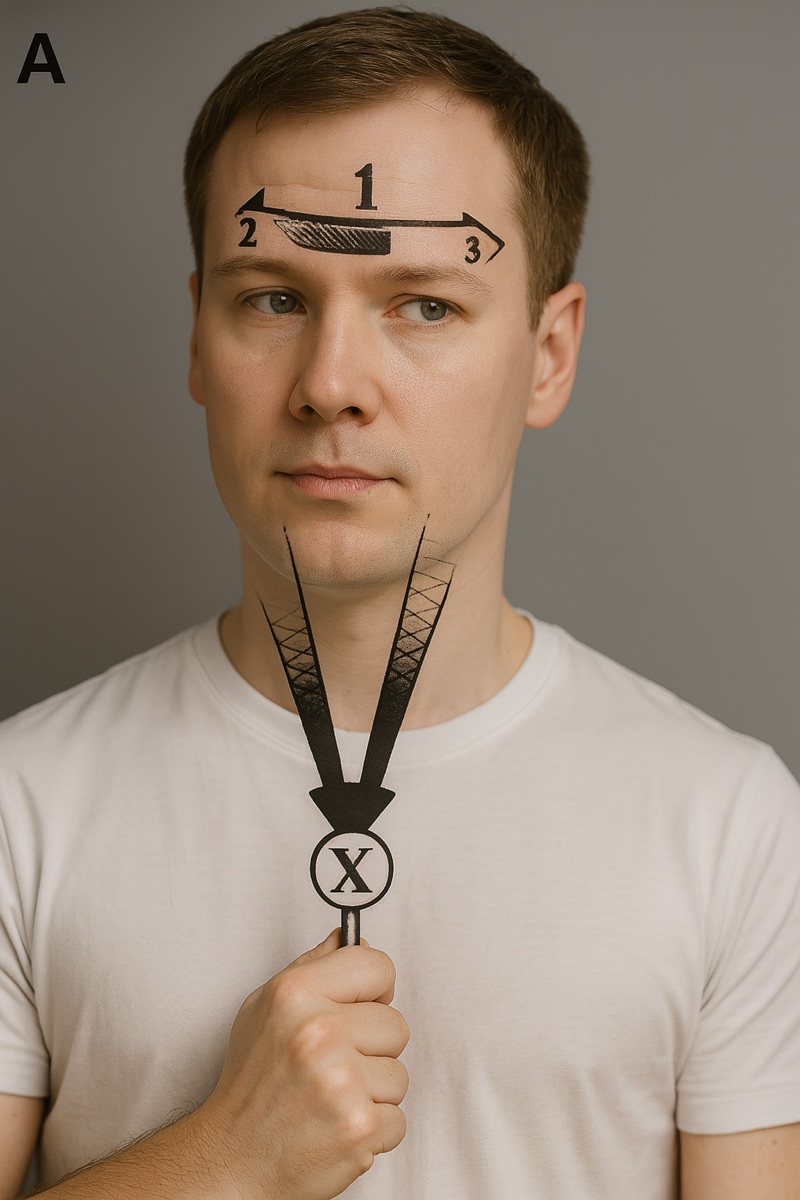
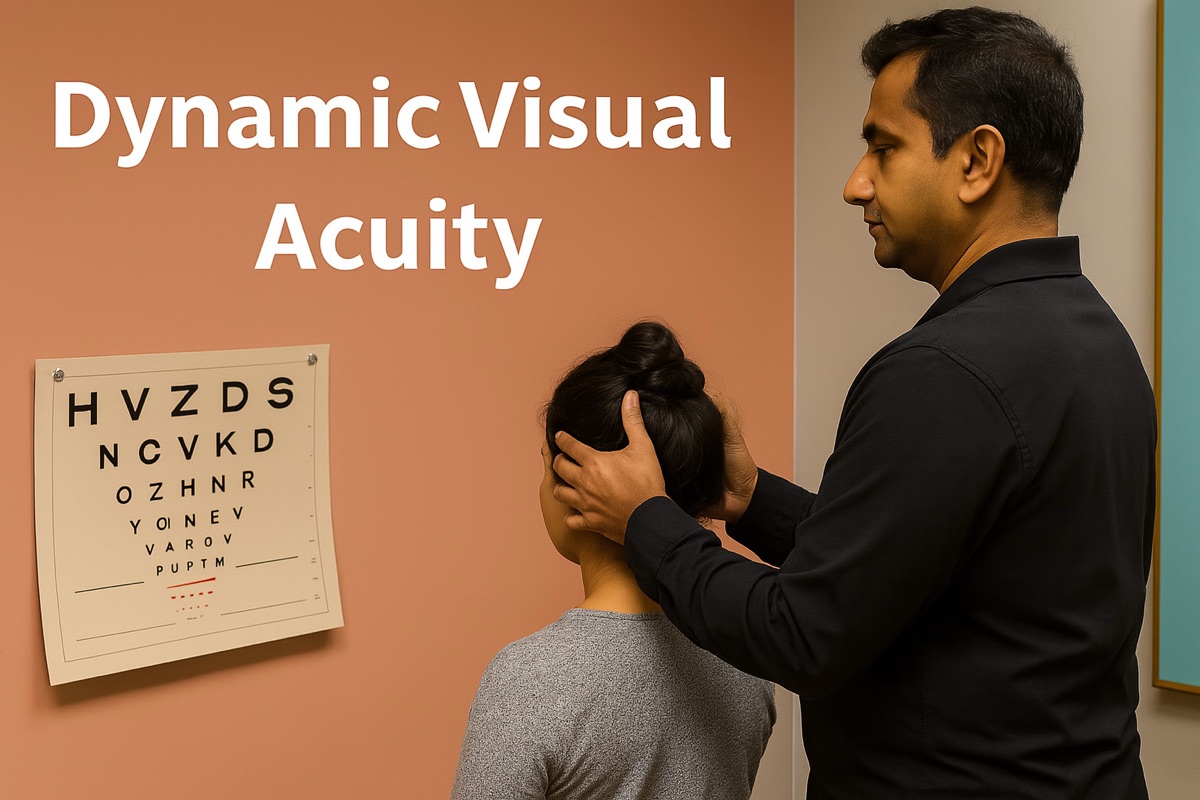
- Gaze instabilityHIT / vHITDynamic Visual AcuityGaze stabilisation (X1 / X2)
- Motion / visual sensitivityVVAShabituation testingHabituation · visual desensitisation
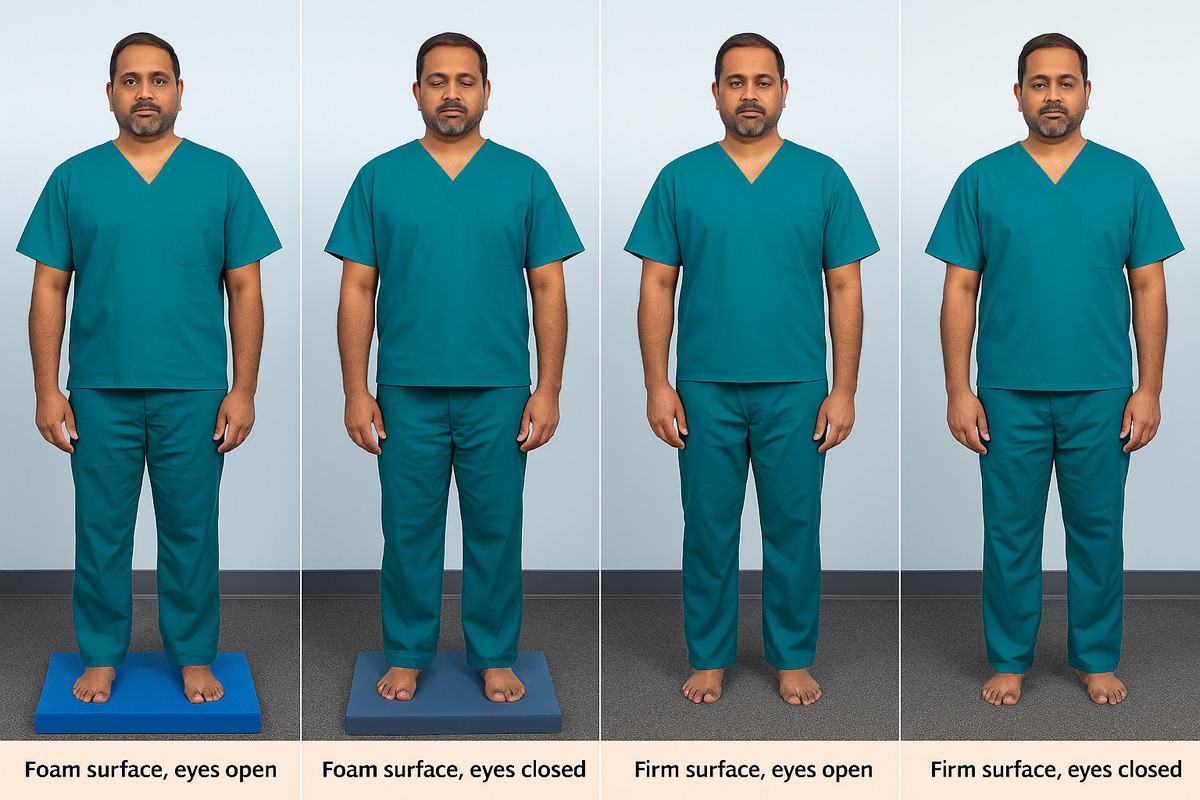
- Postural imbalance · fall riskCDP / SOT · CTSIBBerg · FGA · TUGBalance & gait training
- Self-reported handicapDHIABC scaleTracks progress · sets goals
Subjective scales
The Dizziness Handicap Inventory — 25 items across physical, functional and emotional domains — quantifies perceived handicap and is sensitive to change, making it the workhorse for tracking VRT.1 The ABC scale captures balance confidence (and the psychological side of fall risk), while the Visual Vertigo Analog Scale grades dizziness provoked by visual motion — flagging the visual dependence that points to desensitisation work.2
Objective vestibular & balance testing
The head impulse test (and quantified vHIT) probes semicircular-canal VOR function — a corrective catch-up saccade marks hypofunction and lateralises it.3 Dynamic visual acuity measures gaze stability during head motion, and computerised dynamic posturography (the Sensory Organization Test) quantifies how vestibular, visual and proprioceptive inputs combine — revealing sensory dependence a bedside exam can miss.4 At the bedside, Romberg, tandem gait and the CTSIB (firm vs foam, eyes open/closed) interrogate the same systems without instrumentation.
Functional mobility & fall risk
The Timed Up and Go screens functional mobility — over ~13.5 s flags elevated fall risk in older adults.5 The Berg Balance Scale (14 tasks) and the Functional Gait Assessment (gait under challenge — head turns, obstacles, narrow base) grade postural control and are responsive to rehabilitation, making them ideal repeat measures.6
Re-assessment drives the programme
Beyond classifying the deficit, the baseline carries prognostic weight and sets the schedule for review. Re-running the same validated tools at baseline, mid-treatment (~4–6 weeks) and discharge gives objective evidence to continue, modify or stop — and a weekly symptom diary adds day-to-day pattern and accountability.
Key points
- Classify the deficit: gaze instability (HIT/DVA), motion sensitivity (VVAS), postural imbalance (CDP/BBS/TUG).
- DHI is the workhorse outcome measure; ABC adds balance confidence.
- Low VOR gain + impaired DVA → adaptation; high visual-vertigo scores → habituation.
- Repeat the same tools at ~4–6 weeks to quantify progress objectively.